Well I wanted to see if storing fruit in mason jars really worked. It does and better than I thought.
Started on Monday March 6th today is the 11th. Almost 6 days and the mason jar of bananas are still green. Just starting to ripen.
#banana #masonjarfruitexperiment
Do not do bananas. They look green and you take them out within an hour they start to sweat and turn black. Within 4 hours total glossed over black.
#banana #masonjarbananaexperimentfailure 1
#banana #masonjarbananaexperimentfailure 2
#banana #masonjarbananaexperimentfailure 3
#banana #masonjarbananaexperimentfailure 4
Im also trying the strawberries. 3 weeks ago I bought 16 ounce strawberries. Left them in the refrigerator for about a week or so. They were a little wilted and so I put them in the jar and it actually revived them for another week.
#MasonJarFruitExperiment #Strawberries
Today I bought 3 lbs of strawberries and I put them into the mason jars right away. Storing them in the refrigerator.
Wow who knew that very few people have green eyes. I thought it would have been much higher. Here are some fun facts about green eyes.
Green eyes are the most rare eye color in the world. Only about 2 percent of people in the world have naturally green eyes.
Green eyes are a genetic mutation that results in low levels of melanin, though more melanin than in blue eyes.
Green eyes don’t actually have any color. While green eyes appear to observer as green, the irises themselves have no actual pigment.
86 percent is the highest concentration of people with green eyes and they are found in Ireland, Scotland, and northern Europe.
Sixteen separate genes have been identified as contributing to eye color. So, no matter what eye color your parents have, yours could end up being just about any color. Green eyes naturally occur in all races of people.
There is a village in China called Liqian, in which two-thirds of all inhabitants today have green eyes and blonde hair.
Green eyes and blonde hair are a rare combination.
Every baby is born with either brown or blue eyes. It can take between six months and three years for children to develop green eyes.
Because green eyes have less melanin than brown eyes, people with green eyes are more likely to be extra sensitive to UV rays. The more melanin, the better protection from the sun.
As we all know by now Mauna Loa volcano on the island of Hawaii has erupted.
A woman had reported 2 weeks prior to the eruption of Mauna Loa volcano she had been having earaches. She said she hadn’t had an earache in years. She reported not having had one since the day of the eruption.
Atmospheric pressure waves are a notable phenomenon associated with explosive volcanic eruptions.
Each year, one woman dies every 12 hours from pregnancy related causes, and 1 in 10 babies is born preterm.
Healthy Moms, Strong Babies
When you make a contribution, you’re supporting parents throughout their pregnancies and helping to end preventable maternal health risks and death, end preterm birth and close the health equity gap for every family.
Your thinking about growing your own? Prescription in a natural plant.
Flowered Bud
Here are a few steps you can take to get started.
#1 You’ll need seeds
Before you start let’s get everything you’ll need to set up for success.
Seeds (There are several to choose from)
Containers ( seedlings can be planted in sprouting cubes or directly into big pots 5 gallon size).
Soil ( should be light fluffy non fertilized).
Lights ( depending on how many plants, lighting can be as simple as a regular light bulb for the seedlings to Full Spectrum lighting for growth of vegetation and flowering)
pH Tester ( very important pH balance of the water should be between: First weeks: 5.8 – 5.9. Pre-bloom: 6.0 – 6.2. Real bloom: 6.0 – 6.3
Water ( test your water. You can use bottled spring water with no additives.)
Starting your seeds. You’ll need 1 paper towel and a plastic bag or a plate. Good water is necessary for a healthy start.
Place the paper towel in the bowl, plate or plastic bag. Place your seed or seeds in the center. If more than one seed make sure to give plenty of space between the seeds. Gently pour the water over the paper towel and place in a dark place. Check every day. Should only take a couple of days till a little white root appears. Wait until it’s about 1/2 inch long.
Cover it up and water
After the seed germinates wait until it is 1/2” long. Make a hole about 1 inch deep. A pencil eraser is a measuring tool. Place the root down and the seed cap. Lightly place some fluffy dirt on top and water. Set under the lights about 1” inch above seedling. Don’t turn on the lights until the 2 green leaves appear. Then 18 to 20 hours of light per day.
Recently, French Dermatologists revealed that they may have stumbled onto a new COVID-19 symptom.
There are many strains, forms or types of this virus that have all originated from one original virus. It has come in many forms over the years. Animal related to human to slaughtering of millions of chickens throughout the world. Now COVID-19 drops in and kills thousands accross the world. Closes many countries including the USA, right when becoming happy and financially secure once again was actually happening.
We already know the usual symptoms are a dry or constant cough, shortness of breath, fever, flu-like symptoms and headaches. All of these are already proven to be COVID-19 symptoms of a person suffering from the COVID-19 virus.
However, newer symptoms related to the corona virus form COVID-19 are starting to appear as scientists, doctors and experts fighting time to get more information to get a handle on this COVID-19 virus.
Now dermatologists in France have found the virus can cause unusual manifestations on the skin that might signal infection.
According to the New York Post, the French National Union of Dermatologists-Venereologists (SNDV), found dermatological signs like pseudo-frostbite, hives, blisters and persistent redness have been associated with COVID-19. The sudden redness can be painful, said the doctors.
FRANCE – SNDV REPORTS in a press release.: “We are alerting the public and the medical profession in order to detect these potentially contagious patients as quickly as possible. The doctors advised patients to seek medical consultations in the event they experience such symptoms. According to The Hospitalist, skin manifestations were also observed in one-fifth of a group of patients with COVID-19 in the Alessandro Manzoni Hospital in Lecco, in northern Italy.
Honestly, DOES ANYONE KNOW What We Are Dealing With?
REALITY of just how many have died from other virus’s. Why all of a sudden does this virus rate so high on a death scale as “PANDEMIC”?
Corona virus has many different strains reported by CDC.
Human Coronavirus Types
Coronaviruses are named for the crown-like spikes on their surface. There are four main sub-groupings of coronaviruses, known as alpha, beta, gamma, and delta.
Human coronaviruses were first identified in the mid-1960s. The seven coronaviruses that can infect people are:
Common human coronaviruses
229E (alpha coronavirus)
NL63 (alpha coronavirus)
OC43 (beta coronavirus)
HKU1 (beta coronavirus)
Other human coronaviruses
MERS-CoV (the beta coronavirus that causes Middle East Respiratory Syndrome, or MERS)
SARS-CoV (the beta coronavirus that causes severe acute respiratory syndrome, or SARS)
People around the world commonly get infected with human coronaviruses 229E, NL63, OC43, and HKU1.
Sometimes coronaviruses that infect animals can evolve and make people sick and become a new human coronavirus. Three recent examples of this are 2019-nCoV, SARS-CoV, and MERS-CoV.
Timeline: Early 1900s –The avian flu is first identified in Italy.
1961 – The H5N1 strain is isolated in birds in South Africa.
December 1983 – Chickens in Pennsylvania and Virginia are exposed to the avian flu and more than five million birds are killed to stop the disease from spreading.
1997 – Eighteenpeople are infected by the H5N1 strain in Hong Kong, six die. These are the first documented cases of human infection. Hong Kong destroys its entire poultry population, 1.5 million birds.
1999 – Two children in Hong Kong are infected by the H9N2 strain.
February 2003 – Eighty-fourpeople in the Netherlands are affected by the H7N7 strain of the virus, one dies.
February 7, 2004 – Twelve thousand chickens are killed in Kent County, Delaware, after they are found to be infected with the H7 virus.
October 7, 2005 – The avian flu reaches Europe. Romanian officials quarantine a village of about 30 people after three dead ducks there test positive for bird flu.
November 12, 2005 – A one-year-old boy in Thailand tests positive for the H5N1 strain of avian influenza.
November 16, 2005 – TheWorld Health Organization confirms two human cases of bird flu in China, including a female poultry worker who died from the H5N1 strain.
November 17, 2005 – Two deaths are confirmed in Indonesia from the H5N1 strain of avian influenza.
January 1, 2006 – A Turkish teenager dies of the H5N1 strain of avian influenza in Istanbul, and later that week, two of his sisters die.
January 17, 2006 – A 15-year-old girl from northern Iraq dies after contracting bird flu.
February 20, 2006 – Vietnam becomes the first country to successfully contain the disease. A country is considered disease-free when no new cases are reported in 21 days.
March 12, 2006 – Officials in Cameroon confirm cases of the H5N1 strain. The avian flu has now reached four African countries.
March 13, 2006 – The avian flu is confirmed by officials in Myanmar.
May 11, 2006 – Djibouti announces its first cases of H5N1 – several birds and one human.
December 20, 2011 – The US Department of Health and Human Services releases a statement saying that the government is urging scientific journals to omit details from research they intend to publish on the transfer of H5N1 among mammals. There is concern that the information could be misused by terrorists.
July 31, 2012 – Scientists announce that H3N8, a new strain of avian flu, caused the death of more than 160 baby seals in New England in 2011.
.January 15, 2016 – The US Department of Agriculture confirms that a commercial turkey farm in Dubois County, Indiana, has tested positive for the H7N8 strain of avian influenza.
January 24, 2017 – Britain’s Department for Environment, Food & Rural Affairs releases a statement confirming that a case of H5N8 avian flu has been detected in a flock of farmed breeding pheasants in Preston, UK. The flock is estimated to contain around 10,000 birds. The statement adds that a number of those birds have died, and the remaining live birds at the premises are being “humanely” killed because of disease.
February 12, 2017 – A number of provinces in China have shut down their live poultry markets to prevent the spread of avian flu after a surge in the number of infections from the H7N9 strain. At least six provinces have reported human cases of H7N9 influenza this year, according to Chinese state media, Xinhua.
On 10 August 2010, the World Health Organization declared the H1N1 influenza pandemic over, saying worldwide flu activity had returned to typical seasonal patterns.
WOW did you ever hear anything hear about that one… Nope Did they shut down the country? NOPE
An influenza pandemic is a global outbreak of a new influenza A virus that is very different from current and recently circulating human seasonal influenza A viruses. Influenza A viruses are constantly changing, making it possible on very rare occasions for non-human influenza viruses to change in such a way that they can infect people easily and spread efficiently from person to person.
Pigs experimentally infected with the strain of swine flu that caused the human pandemic of 2009–10 showed clinical signs of flu within four days, and the virus spread to other uninfected pigs housed with the infected ones and then to humans.
1940s: Thomas Francis, Jr., MD and Jonas Salk, MD serve as lead researchers at the University of Michigan to develop the first inactivated flu vaccine with support from the U.S. Army. Their vaccine uses fertilized chicken eggs in a method that is still used to produce most flu vaccines today. The Army is involved with this research because of their experience with troop loss from flu illness and deaths during WWI. This original vaccine only includes an inactivated influenza A virus.
1940s: First-generation mechanical ventilators become available. These machines support breathing in patients suffering respiratory complications.
1940: Influenza B viruses are discovered.
1942: A bivalent (two component) vaccine that offers protection against influenza A and influenza B viruses is produced after the discovery of influenza B viruses.
1944: Use of cell cultures for virus growth is discovered. This allows viruses to be cultured outside the body for the first time. The ability to culture influenza from respiratory secretions allows diagnosis of influenza.
1945: Inactivated influenza vaccine is licensed for use in civilians.
1942: The Communicable Disease Center (CDC) opens in the old offices of the Malaria Control in War Areas, located on Peachtree Street in Atlanta, Georgia with a satellite campus in Chamblee. Launched with fewer than 400 employees, the organization—today the Centers for Disease Control and Prevention–moves to its current main campus on Clifton Road in Atlanta in 1947 after paying $10 to Emory University for 15 acres of land.
1947: During the seasonal flu epidemic of 1947, investigators determine that changes in the antigenic composition of circulating influenza viruses has rendered existing vaccines ineffective, highlighting the need for continuous surveillance and characterization of circulating flu viruses.
1948: The World Health Organization (WHO) Influenza Centre is established at the National Institute for Medical Research in London. The primary tasks of the organization are to collect and characterize influenza viruses, develop methods for the laboratory diagnosis of influenza virus infections, establish a network of laboratories, and disseminate data accumulated from their investigations.
1950s
1952: The Global Influenza Surveillance and Response System (GISRS) is created by WHO to monitor the evolution of influenza viruses. The GISRS network originally includes 26 laboratories.
1956: The CDC’s Influenza Branch in Atlanta is designated a WHO Collaborating Centre for Surveillance, Epidemiology & Control of Influenza.
1957: A new H2N2 flu virus emerges to trigger a pandemic. There are about 1.1 million deaths globally, with about 116,000 in the U.S.
1960s
1960: In 1960, the US Surgeon General, in response to substantial morbidity and mortality during the 1957–58 pandemic, recommends annual influenza vaccination for people with chronic debilitating disease, people aged 65 years or older, and pregnant women.
1961: An outbreak in South Africa raises possibility of wild birds as a possible reservoir for influenza A viruses.
1962: CDC launches the 122 Cities Mortality Reporting System. Each week, the vital statistics office of 122 cities across the U.S. report the total number of death certificates processed and the number of those for which pneumonia or influenza is listed as an underlying or contributing cause of death by age group. The system is retired in October 2016.
1966: The FDA licenses amantadine, a new antiviral medication, as a prophylactic (preventive medicine) against influenza A. It isn’t effective against influenza B.
1967: Dr. H.G. Pereira and colleagues propose a relationship between human and avian flu viruses after a study shows an antigenic relationship between the 1957 human pandemic A virus and an influenza A virus isolated from a turkey. The study raises the question and triggers the body of work on whether human influenza viruses are of avian origin.
1968: A new H3N2 influenza virus emerges to trigger another pandemic, resulting in roughly 100,000 deaths in the U.S. and 1 million worldwide. Most of those deaths are in people 65 and older. H3N2 viruses circulating today are descendants of the H3N2 virus that emerges in 1968.
1970s
An H1N1 (swine flu) outbreak among recruits at Fort Dix leads to a vaccination program to prevent a pandemic. Within 10 months, roughly 25% of the US population is vaccinated (48 million people), about twice the level needed to provide coverage for the at-risk population. Cases of Guillain-Barre syndrome, a neurologic condition that in rare instances has been associated with vaccination, among vaccine recipients appeared to be in excess of what was expected, so officials determine the vaccination program should be halted. 1981: CDC begins collecting reports of influenza outbreaks from state and territorial epidemiologists.
Initially, infected foreign nationals were turned back at the U.S. border to help prevent additional infections. The number of U.S. deaths from AIDS have declined sharply since the early years of the disease’s presentation domestically. In the United States in 2016, 1.1 million people aged over 13 lived with an HIV infection, of whom 14% were unaware of their infection.
As of 2016, about 675,000 people have died of HIV/AIDS in the U.S. since the beginning of the HIV epidemic, and even today, nearly 13,000 people with AIDS in the United States die each year. [3]
With improved treatments and better prophylaxis against opportunistic infections, death rates have quite significantly declined.[4]
The overall death rate among persons diagnosed with HIV/AIDS in New York City decreased by sixty-two percent from 2001 to 2012.
1990s
1993: The Vaccines for Children (VFC) Program is established as a result of a measles outbreak to provide vaccines at no cost to children whose parents or guardians might not be able to afford them. The program increases the likelihood of children getting recommended vaccinations on schedule.
1993: The costs of influenza vaccine become a covered benefit under Medicare Part B.
1994: Rimantadine, derived from amantadine, is approved by the FDA to treat influenza A.
1996: An avian influenza H5N1 virus is first isolated from a farmed goose in China.
1997: The first human infection with an avian influenza A H5N1 virus is identified in Hong Kong.
1997: FluNet, a web-based flu surveillance tool, is launched by WHO. It is a critical tool for tracking the movement of flu viruses globally. Country data is updated weekly and is publically available.
1998: Influenza virus surveillance in swine, conducted by the US Department of Agriculture, begins in the United States. A virus that is a hybrid of human, bird and swine flu viruses is detected in pigs. This virus becomes the dominant flu virus in U.S. pigs by 1999.
1999: A pandemic planning framework is published by WHO emphasizing the need to enhance influenza surveillance, vaccine production and distribution, antiviral drugs, influenza research and emergency preparedness
1999: The neuraminidase inhibitors oseltamivir (Tamiflu®) and zanamivir (Relenza®) are licensed to treat influenza infection.
2000s
April 2002: The Advisory Committee on Immunization Practices (ACIP) encourages that children 6 to 23 months of age be vaccinated annually against influenza.
2003: Public health officials are concerned about a re-emergence of H5N1 avian influenza reported in China and Vietnam.
June 2003: The first nasal spray flu vaccine is licensed.
2004: The National incident Management System (NIMS) is established to coordinate response for public health incidents that require actions by all levels of government, as well as public, private, and nongovernmental organizations.
2005: The US. Government National Strategy for Pandemic Influenza is published
2005: The entire genome of the 1918 H1N1 pandemic influenza virus is sequenced
2006: CDC stops recommending adamantanes during the 2005-2006 season after high levels of resistance among influenza A viruses. In the US, resistance increased from 1.9% during the 2003-2004 season to 11% in the 2004-2005 season.
2006: The National Strategy for Pandemic Influenza Implementation Plan is published. The document outlines U.S. preparedness and response to prevent the spread of a pandemic.
2007: The American Veterinary Medical Association (AVMA) establishes the One Health initiative Task Force, an effort to attain optimal health for people, animals, and the environment.
2007: The American Medical Association unanimously approves a resolution calling for increased collaboration between human and veterinary medical communities. The term ‘one health,’ which looks at the interactions between animal and human health, enters the medical and scientific lexicon.
2007: The One Health approach is recommended for pandemic preparedness during the International Ministerial Conference on Avian and Pandemic Influenza
2007: FDA approves the first U.S. vaccine for people against an avian influenza A(H5N1) virus.
2007: Human infection with a novel influenza virus is added to the nationally notifiable disease list
2008: ACIP expands its influenza vaccination recommendation to include vaccination of children ages 5-18 years.
2008: HHS Pandemic Influenza Operational Plan is published
2008: CDC receives US Food and Drug Administration approval for a highly sensitive influenza polymerase chain reaction (PCR) assay. These tests can detect influenza with high specificity that enhances diagnosis and treatment options.
2008: The Influenza Reagent Resource (IRR) is established by CDC to provide registered users with reagents, tools, and information to study and detect influenza viruses
April 17, 2009: A new H1N1 virus is detected in the U.S.
CDC begins working to develop a virus (called a candidate vaccine virus) that could be used to make vaccine to protect against this new virus.
April 25, 2009: The World Health Organization (WHO) declares a public health emergency of international concern.
June 11, 2009: WHO officially declares the new 2009 H1N1 outbreak a pandemic.
2009: Physicians use point of care rapid immunoassay tests to provide influenza results within 15 minutes during the H1N1 pandemic
October 5, 2009: The first doses of monovalent H1N1 pandemic vaccine are administered.
2010s
August 10, 2010: WHO declares an end to 2009 H1N1 influenza pandemic.
2010: The ACIP recommends annual influenza vaccination for those 6 months of age and older.
2012: Vaccines containing cell-cultured virus become available. Even though eggs continue to be the primary means of production, cell culture emerges as an alternative method for producing influenza vaccines.
2012: WHO makes first vaccine composition recommendation for a quadrivalent vaccine.
2012: CDC partners with Association of Public Health laboratories to define the optimal right size for influenza virologic surveillance. The project produces right-size calculators; statistical tools that help states determine the optimal amount of influenza testing needed for desired confidence levels of surveillance.
2014: The FDA approves peramivir (Rapivab) to treat influenza in adults. It is the first IV flu medication.
2017: CDC updates guidelines for use of non-pharmaceutical measures to help prevent spread of pandemic influenza based on latest scientific evidence. These are actions that individuals and communities can take to help slow spread of the flu like staying home when sick, covering a cough or sneeze, and frequently washing hands.
Get The Answers You Need About Your Pets and COVID-19 With Dr. Karen Becker
It’s important to keep in mind that at the present time this is an ever-evolving situation rife with competing theories and conspiracies, widespread mis- and disinformation, politics, etc. My goal today is to update you about what we know at this point regarding COVID-19 and furry family members.
Animals and COVID-19
According to veterinary publication dvm360, there are reports of animals being abandoned or killed because their owners fear they might harbor COVID-19.1 This is an absolutely unnecessary and tragic situation.
While it’s clear we’re still learning about this virus, at this time the WHO website maintains this particular type of coronavirus can be transmitted from human to human. From the OIE World Organisation for Animal Health Questions and Answers on the 2019 Coronavirus Disease (COVID-19) webpage:2
“Are animals responsible for COVID-19 in people?
The predominant route of transmission of COVID-19 appears to be from human to human.
Current evidence suggests that the COVID-19 virus has an animal source. Ongoing investigations are important for identifying the animal source (including species involved) and establishing the potential role of an animal reservoir in this disease. Yet, to date, there is not enough scientific evidence to identify that source or to explain the route of transmission from an animal source to humans.
Genetic sequence data reveals that the COVID-19 virus is a close relative of other CoV found circulating in Rhinolophus bat (Horseshoe Bat) populations. There is the possibility that transmission to humans involved an intermediate host.
Priorities for research to investigate the animal source were discussed by the OIE informal advisory group on COVID-19 and were presented at the WHO Global Research and Innovation Forum (11-12 February 2020) by the President of the OIE Wildlife Working Group. The outcomes from the discussion of the OIE informal advisory group on COVID-19 can be found at the link.”
Pets, COVID-19, and Confirmed Infection in One Dog in Hong Kong
Also from the OIE World Organisation for Animal Health Questions and Answers on the 2019 Coronavirus Disease (COVID-19) webpage:3
“What do we know about COVID-19 virus and companion animals?
The current spread of COVID-19 is a result of human to human transmission. To date, there is no evidence that companion animals can spread the disease. Therefore, there is no justification in taking measures against companion animals which may compromise their welfare.
The Veterinary Services of the Hong Kong Special Administrative Region of the People’s Republic of China reported to OIE evidence that a dog had tested positive to the COVID-19 virus following close exposure to its owners who were sick with COVID-19 – see Immediate Notification (03/01/2020) and Follow-up report no.1 (03/08/2020).
The test, conducted by real time PCR, showed the presence of genetic material from the COVID-19 virus. The dog [a 17-year-old Pomeranian] was not showing any clinical signs of the disease.
There is no evidence that dogs play a role in the spread of this human disease or that they become sick. Further studies are needed to understand if and how different animals could be affected by COVID-19 virus. The OIE will continue to provide updates as new information becomes available.
There is no evidence to support restrictions to movement or trade of companion animals.”
According to a post on March 9th in PetfoodIndustry.com:
“Veterinarians confirmed that the coronavirus had infected the dog too after taking nasal, oral and rectal swabs, along with fecal samples. The World Organization for Animal Health (OIE) published a report of the emerging disease, listing this case as the first known in dogs.
Nasal and oral samples tested positive for the presence of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the name of virus responsible for COVID-19. However, the dog hasn’t shown any outward signs of illness. Follow-up oral and nasal samples taken on March 2 and 5 continues to test positive.
Doctors and veterinarians don’t know if the COVID-19 virus has the potential to be zoonotic, or transmitted from dogs to people.
Doctors don’t know if the dog got the virus directly from its owner, or through an intermediary species. Likewise, doctors don’t know how the virus was transmitted to the dog, whether by airborne particles, direct contact or bodily fluids.
In Hong Kong, health authorities quarantine mammalian pets from households with confirmed human cases of COVID-19 and place the animals under veterinary surveillance for 14 days, according to the report.”4
Why Pet Parents Should NOT Hit the Panic Button
Many veterinarians have called for calm after the announcement, reminding owners this doesn’t mean dogs can get sick from the virus or transmit it back to humans. Panic makes people do foolish, regrettable things, which is what has occurred in Wuhan. From a March 4th post in the Whole Dog Journal:
“Tragically, within days [of the report of the single infected dog], there were reports of a record number of dogs and other pets being abandoned in China’s streets, and thousands of pets being surrendered to overwhelmed animal shelters — despite the fact that there is no indication that the COVID-19 virus is zoonotic.
Time magazine reports that the crisis for pet dogs and cats is the worst in Wuhan, the capital city of the Hubei province where the first cases of COVID-19 are believed to have emerged. Time reports that when a person in Wuhan is found to have COVID-19, the authorities kill all animals in the home as a precaution.
This report was corroborated by a reporter for the BBC (British news service):
‘Volunteers in China say they’re struggling to keep up with the number of animals being abandoned as the country battles the virus outbreak. More than 2,000 people in China have died and more than 78,000 infections have been reported in the country.
Pet owners who fall sick or are caught up in quarantine can’t take their animals with them, and despite reassurance from the World Health Organization that animals can’t carry the virus, others are being dumped.’”5
The Centers for Disease Control is now advising people with COVID-19 to avoid close contact with their pets, but on February 28th, Dr. Jonathan Ball at the University of Nottingham has called the widespread panic about the news “incredibly irresponsible”:
“There is no evidence that the human novel coronavirus can infect dogs and it would be incredible for a virus to make so many species jumps in such a short space of time!
We have to differentiate between real infection and just detecting the presence of a virus – these are very different – and the fact that the test result was weakly positive would suggest that this is environmental contamination or simply the presence of coronavirus shed from the human contact that has ended up in the dog’s samples.
In truth this is incredibly irresponsible because the last thing we need to do is create mass hysteria about the possibility of dogs being infected, and therefore potentially transmitting this virus when there is absolutely no evidence for this whatsoever.”6
If You’re a Pet Parent, Do This Instead
From the American Veterinary Medical Association (AVMA) COVID-19 website:
“The precise meaning of the positive test result from the one dog remains unclear and further evaluation is ongoing. Hong Kong officials said that dog continues to show no clinical signs of illness, remains under quarantine and is being cared for, and will continue to be monitored and tested.
We will keep you updated you as we learn more. At this time, the CDC, the World Health Organization (WHO), and the World Organisation for Animal Health (OIE) say there is no evidence that companion animals, including pets, spread COVID-19.
As always, it’s a good idea to wash your hands after being around animals, and animal owners should continue to include pets and other animals in their emergency preparedness planning, including keeping a two-week supply of food and medications on hand.”7
If someone in your household is diagnosed with the virus and you feel additional precautions are necessary, the following is from the CDC:
“Considerations for COVID-19 patients under home care and isolation who have pets or other animals:
People with COVID-19 should be advised to tell their public health point of contact that they have pets or other animals in their home.
In addition to other prevention measures, people with COVID-19 who are identified by public health officials as requiring home care and isolation should be advised to limit interaction with pets and other animals.
Specifically, while these people are symptomatic, they should maintain separation from pets as they would with other household members, and avoid direct contact with pets, including petting, snuggling, being kissed or licked, and sharing food. Service animals should be permitted to remain with their handlers.
If possible, a household member should be designated to care for pets in the home. If the individual in home care and isolation must care for pet(s), including service animals, they should ensure they wash their hands before and after caring for pets and wear a facemask while interacting with pets, until they are medically cleared to return to normal activities.”8
Nature to the Rescue?
The race is on to not only learn more about how COVID-19 affects other species but for biotech companies to produce a slew of pharmaceutical products in response to this latest disease outbreak.
Interestingly, the most accessible and effective treatment may already exist at your local health food store. Dr. Michel Chrétien’s Montreal laboratory is testing quercetin, an all-natural extract from plants, and its derivatives, as a possible “broad spectrum” antiviral medication. Clinical trials began in China a few weeks ago.9
The FDA has stated that CBD is not a treatment for serious illnesses such as cancer, Diabetes and Alzeheimer’s.
CBD can take any where from 30 minutes to four hours to take effect. The effects can last up to 6 to 8 hours.
Over Dosing America
So if that chewy cookie contains 30 milligrams and the adult reccomended adult dosage is 5 milligrams, if you eat the entire cookie you will be over dosing yourself.
What CBD does treat is in lotions for pain releif, tinctures for pain relief and stomach issues. These products along with the edibles have been said to releive many ailments.
Recreational Users: Dont be fooled about the potency. If you are inhaling THC from smoking the product, edibles with CBD is much more potent and a different “High”.
Where THC can treat MANY bI pOLAR, aNXIETY, pANIC aTTACK mental issues by just smoking to calm someone
Cancer patients use THC by consuming and smoking the product. Patients releave nausea and increase their apatite also by smoking.
Over the past decade, the cannabis- and hemp-derived compound cannabidiol (CBD) as well as other cannabinoids have taken center stage in the ongoing revolution of natural medicine. This is mostly due to the work of medical researchers, who through numerous independent studies have found evidence of various medicinal and therapeutic properties in CBD. Today, both natural and synthetic CBD is commonly used around the world to ameliorate symptoms of a wide variety of disorders. These include:
Chronic pain disorders such as arthritis
Seizures and epilepsy
Sleep disorders and insomnia
Inflammatory disorders such as gout or IBD
Anxiety disorders
Vascular and circulatory problems
It’s worth noting that evidence of CBD’s potential health benefits recorded in scientific literature are from studies analyzing pharmaceutical-grade CBD, which is very different from the CBD products available to the public. As of this writing, there is only one CBD oil approved by the FDA for prescription: a product called Epidiolex. Physicians are still generally hesitant to prescribe CBD, and usually recommend it as a supplementary form of home medication.
Naturally-Sourced CBD: Where It Comes From & Why That’s a Good Thing
Aside from the work of medical researchers, there is an impressive amount of anecdotal evidence supporting the idea that naturally-sourced CBD productscan reduce or improve the severity of symptoms related to a variety of conditions; from panic attacks to obsessive compulsive disorder.
Some independent studies have even found that naturally-sourced CBD can cause appreciable improvement in symptoms related to the early stages of dementia, such as mood swings, aggravation and disruption of circadian rhythms. This is due in large part to the fact that natural CBD comes from two plants chock-full of health-positive compounds: cannabis and hemp.
The Dangers of Synthetic CBD & Natural Cannabinoid Analogs
With the skyrocketing popularity of the legal whole-plant cannabis industry, several companies have sought to simultaneously increase profits and reduce production time by creating synthetic CBD and cannabinoids. These are man-made chemicals typically synthesized with either fluoride or bromide, and designed to emulate the effects of naturally-sourced CBD and cannabinoids. They are then touted as “just as effective” with “no side effects.”
A key study by the Journal of Medical Phyto Research in Los Gatos, California analyzed the catabolic enzyme production of two control groups over 22 weeks; the first taking natural CBD and the second taking synthetic CBD. The second group showed dangerous levels of Alanine Amino Transferase (ALT) and Aspartate Amino Transferase (AST), two enzymes recruited to remove the synthetic CBD from their bodies. The study concluded that the human body is not equipped to properly catabolize synthetic cannabinoids.
In the summer of 2018, the FDAissued a statement warning of the “significant health risks of synthetic cannabinoid products” and linked their usage to “severe illnesses and even deaths” in several cases over the past few months in a number of states across America.
Coronaviruses are common in many different species of animals, including camels and bats. Rarely, these coronaviruses can evolve and infect humans and then spread between humans. Recent examples of this include SARS-CoV and MERS-CoV.
Most coronaviruses infect animals, but not people. In the future, one or more of these other coronaviruses could potentially evolve and spread to humans, as has happened in the past. We still don’t understand why only certain coronaviruses are able to infect people.
Common human coronaviruses
Common human coronaviruses, including types 229E, NL63, OC43, and HKU1, usually cause mild to moderate upper-respiratory tract illnesses, like the common cold. Most people get infected with these viruses at some point in their lives. These illnesses usually only last for a short amount of time. Symptoms may include
runny nose
headache
cough
sore throat
fever
a general feeling of being unwell
Human coronaviruses can sometimes cause lower-respiratory tract illnesses, such as pneumonia or bronchitis. This is more common in people with cardiopulmonary disease, people with weakened immune systems, infants, and older adults.
Transmission
Human coronaviruses most commonly spread from an infected person to others through
the air by coughing and sneezing
close personal contact, such as touching or shaking hands
touching an object or surface with the virus on it, then touching your mouth, nose, or eyes before washing your hands
rarely, fecal contamination
In the United States, people usually get infected with common human coronaviruses in the fall and winter. However, you can get infected at any time of the year. Most people will get infected with one or more of the common human coronaviruses in their lifetime. Young children are most likely to get infected. However, people can have multiple infections in their lifetime.
Other human coronaviruses
Most people confirmed to have MERS-CoV infection have had severe respiratory illness with symptoms of:
fever
cough
shortness of breath
Some people also had diarrhea and nausea/vomiting. For many people with MERS, more severe complications followed, such as pneumonia and kidney failure. About 3 or 4 out of every 10 people reported with MERS have died. Most of the people who died had a pre-existing medical condition that weakened their immune system, or an underlying medical condition that hadn’t yet been discovered. Medical conditions sometimes weaken people’s immune systems and make them more likely to get sick or have severe illness.
Pre-existing conditions among people who got MERS have included
diabetes
cancer
chronic lung disease
chronic heart disease
chronic kidney disease
Some infected people had mild symptoms (such as cold-like symptoms) or no symptoms at all.
The symptoms of MERS start to appear about 5 or 6 days after a person is exposed, but can range from 2 to 14 days.
The coronavirus that originated in Wuhan, China, raised global concerns but, after a two day meeting, the World Health Organization has issued a statement saying the situation is not yet an emergency of international concern.
Meanwhile, the Centers for Disease Control and Prevention is monitoring the situation and will provide updated information as it becomes available. In addition, Mayo Clinic continues to closely monitor the coronavirus outbreak and says staff is trained and prepared to care for patients, should the need arise. Dr. Pritish Tosh, a Mayo Clinic infectious diseases specialist, says health care providers need to ask patients with respiratory illness and fever about their recent travel. “It’s important we focus on patients with fever and respiratory symptoms, not just for the novel coronavirus, but also for other respiratory viruses that are circulating, such as influenza,” says Dr. Tosh. “Once these patients are identified, they should be given a mask to wear and put into a room where a health care provider can ask them about recent travel.” Dr. Tosh adds, “They may have been to a part of the Middle East where there is ongoing MERS (Middle East respiratory syndrome) infections. They may also have been in Wuhan, China, or been close to someone who has been there.” The coronavirus is in the same family of viruses as SARS (severe acute respiratory syndrome) and MERS.
People with an increased risk of lung cancer may consider annual lung cancer screening using low-dose CT scans. Lung cancer screening is generally offered to people 55 and older who smoked heavily for many years and are otherwise healthy.
Discuss your lung cancer risk with your doctor. Together you can decide whether lung cancer screening is right for you.
Tests to diagnose lung cancer
If there’s reason to think that you may have lung cancer, your doctor can order a number of tests to look for cancerous cells and to rule out other conditions.
Tests may include:
Imaging tests. An X-ray image of your lungs may reveal an abnormal mass or nodule. A CT scan can reveal small lesions in your lungs that might not be detected on an X-ray.
Sputum cytology. If you have a cough and are producing sputum, looking at the sputum under the microscope can sometimes reveal the presence of lung cancer cells.
Tissue sample (biopsy). A sample of abnormal cells may be removed in a procedure called a biopsy. Your doctor can perform a biopsy in a number of ways, including bronchoscopy, in which your doctor examines abnormal areas of your lungs using a lighted tube that’s passed down your throat and into your lungs; mediastinoscopy, in which an incision is made at the base of your neck and surgical tools are inserted behind your breastbone to take tissue samples from lymph nodes; and needle biopsy, in which your doctor uses X-ray or CT images to guide a needle through your chest wall and into the lung tissue to collect suspicious cells. A biopsy sample may also be taken from lymph nodes or other areas where cancer has spread, such as your liver.
Careful analysis of your cancer cells in a lab will reveal what type of lung cancer you have. Results of sophisticated testing can tell your doctor the specific characteristics of your cells that can help determine your prognosis and guide your treatment.
Tests to determine the extent of the cancer
Once your lung cancer has been diagnosed, your doctor will work to determine the extent (stage) of your cancer. Your cancer’s stage helps you and your doctor decide what treatment is most appropriate.
Staging tests may include imaging procedures that allow your doctor to look for evidence that cancer has spread beyond your lungs. These tests include CT, MRI, positron emission tomography (PET) and bone scans. Not every test is appropriate for every person, so talk with your doctor about which procedures are right for you.
The stages of lung cancer are indicated by Roman numerals that range from 0 to IV, with the lowest stages indicating cancer that is limited to the lung. By stage IV, the cancer is considered advanced and has spread to other areas of the body.
You and your doctor choose a cancer treatment plan based on a number of factors, such as your overall health, the type and stage of your cancer, and your preferences.
In some cases, you may choose not to undergo treatment. For instance, you may feel that the side effects of treatment will outweigh the potential benefits. When that’s the case, your doctor may suggest comfort care to treat only the symptoms the cancer is causing, such as pain or shortness of breath.
Surgery
During surgery your surgeon works to remove the lung cancer and a margin of healthy tissue. Procedures to remove lung cancer include:
Wedge resection to remove a small section of lung that contains the tumor along with a margin of healthy tissue
Segmental resection to remove a larger portion of lung, but not an entire lobe
Lobectomy to remove the entire lobe of one lung
Pneumonectomy to remove an entire lung
If you undergo surgery, your surgeon may also remove lymph nodes from your chest in order to check them for signs of cancer.
Surgery may be an option if your cancer is confined to the lungs. If you have a larger lung cancer, your doctor may recommend chemotherapy or radiation therapy before surgery in order to shrink the cancer. If there’s a risk that cancer cells were left behind after surgery or that your cancer may recur, your doctor may recommend chemotherapy or radiation therapy after surgery.
Radiation therapy
Radiation therapy uses high-powered energy beams from sources such as X-rays and protons to kill cancer cells. During radiation therapy, you lie on a table while a machine moves around you, directing radiation to precise points on your body.
For people with locally advanced lung cancer, radiation may be used before surgery or after surgery. It’s often combined with chemotherapy treatments. If surgery isn’t an option, combined chemotherapy and radiation therapy may be your primary treatment.
For advanced lung cancers and those that have spread to other areas of the body, radiation therapy may help relieve symptoms, such as pain.
Chemotherapy
Chemotherapy uses drugs to kill cancer cells. One or more chemotherapy drugs may be given through a vein in your arm (intravenously) or taken orally. A combination of drugs usually is given in a series of treatments over a period of weeks or months, with breaks in between so that you can recover.
Chemotherapy is often used after surgery to kill any cancer cells that may remain. It can be used alone or combined with radiation therapy. Chemotherapy may also be used before surgery to shrink cancers and make them easier to remove.
In people with advanced lung cancer, chemotherapy can be used to relieve pain and other symptoms.
Radiosurgery
Stereotactic body radiotherapy, also known as radiosurgery, is an intense radiation treatment that aims many beams of radiation from many angles at the cancer. Stereotactic body radiotherapy treatment is typically completed in one or a few treatments.
Radiosurgery may be an option for people with small lung cancers who can’t undergo surgery. It may also be used to treat lung cancer that spreads to other parts of the body, including the brain.
Targeted drug therapy
Targeted drug treatments focus on specific abnormalities present within cancer cells. By blocking these abnormalities, targeted drug treatments can cause cancer cells to die.
Many targeted therapy drugs are used to treat lung cancer, though most are reserved for people with advanced or recurrent cancer.
Some targeted therapies only work in people whose cancer cells have certain genetic mutations. Your cancer cells may be tested in a laboratory to see if these drugs might help you.
Immunotherapy
Immunotherapy uses your immune system to fight cancer. Your body’s disease-fighting immune system may not attack your cancer because the cancer cells produce proteins that blind the immune system cells. Immunotherapy works by interfering with that process.
Immunotherapy treatments are generally reserved for people with advanced lung cancer.
Palliative care
People with lung cancer often experience signs and symptoms of the cancer, as well as side effects of treatment. Supportive care, also known as palliative care, is a specialty area of medicine that involves working with a doctor to minimize your signs and symptoms.
Your doctor may recommend that you meet with a palliative care team soon after your diagnosis to ensure that you’re comfortable during and after your cancer treatment.
In one study, people with advanced non-small cell lung cancer who began receiving supportive care soon after their diagnosis lived longer than those who continued with treatments, such as chemotherapy and radiation. Those receiving supportive care reported improved mood and quality of life. They survived, on average, almost three months longer than did those receiving standard care.
Proton therapy is a type of radiation therapy — a treatment that uses high-energy beams to treat tumors. Radiation therapy using X-rays has long been used to treat cancers and noncancerous (benign) tumors. Proton therapy is a newer type of radiation therapy that uses energy from positively charged particles called protons.
Proton therapy has shown promise in treating several kinds of cancer. Studies have suggested that proton therapy may cause fewer side effects than traditional radiation, since doctors can better control where the proton beams deposit their energy. But few studies have directly compared proton therapy radiation and X-ray radiation, so it’s not clear whether proton therapy is more effective in prolonging lives.
Proton therapy isn’t widely available in the United States.
This is the machine that delivers the treatment.
Why it’s done
Proton therapy is used as a treatment for cancer and some noncancerous tumors. Proton therapy may be used as the only treatment for your condition. Or it may be used in conjunction with other treatments, such as surgery and chemotherapy.
Proton therapy is sometimes used to treat:
Brain tumors
Breast cancer
Cancer in children
Eye melanoma
Esophageal cancer
Head and neck cancers
Liver cancer
Lung cancer
Pituitary gland tumors
Prostate cancer
Sarcoma
Tumors affecting the spine
Tumors in the base of the skull
Clinical trials are investigation proton therapy as a treatment for a number of other types of cancer.
Risks
Proton therapy can cause side effects as the cancer cells die or when the energy from the proton beam damages healthy tissue.
Because doctors can better control where proton therapy releases its highest concentration of energy, proton therapy is believed to affect less healthy tissue and have fewer side effects than traditional radiation therapy. Still, proton therapy does release some of its energy in healthy tissue.
What side effects you experience will depend on what part of your body is being treated and the dose of proton therapy you receive.
In general, common side effects of proton therapy include:
Fatigue
Mouth, eating and digestion problems
Headaches
Hair loss around the part of your body being treated
Skin redness around the part of your body being treated
Soreness around the part of your body being treated
How you prepare
Before you undergo proton therapy, your health care team guides you through a planning process to ensure that the proton beam reaches the precise spot in your body where it’s needed.
Planning typically includes:
Determining the best position for you during treatment. During radiation simulation, your radiation therapy team works to find a comfortable position for you during treatment. It’s imperative that you lie still during treatment, so finding a comfortable position is vital. To do this, you’ll be positioned on a table that will be used during your treatment. Cushions and restraints are used to place you in the correct position and to help you hold still. Your radiation therapy team will mark the area of your body that will receive the radiation. Depending on your situation, you may receive temporary marking with a marker or you may receive permanent tattoos.
Planning the path of the protons with imaging tests. Your radiation therapy team may have you undergo magnetic resonance imaging (MRI) or computerized tomography (CT) scans to determine the area of your body to be treated and how best to reach it with the proton beams.
Consider the cost
Proton therapy is a newer form of radiation therapy that may be more expensive than traditional radiation therapy with X-rays. Not all insurance policies cover proton therapy. When considering your treatment options, work with your health insurance provider to understand what costs are covered by insurance and which costs you’ll be expected to pay.
What you can expect
During proton therapy
You typically undergo proton therapy five days a week for several weeks. However, in some cases, you may undergo only one or only a few treatments, depending on your condition. The actual proton therapy treatment may take only a minute or so, but expect to spend 30 to 45 minutes preparing before each treatment session.
You may also undergo weekly CT verification scans to see if the dose you receive needs to be recalculated based on changes in weight, or tumor size and shape, depending on your situation.
To prepare, you’ll be positioned on a table. Cushions and restraints will be used to hold your body still. Then you’ll undergo an imaging test, such as an X-ray or CT scan, to make sure your body is in the same precise position before each treatment.
Your radiation therapy team will then leave the room and go to an area where they can monitor you. They can still see and hear you.
What you experience next depends on the type of proton therapy machine your treatment team uses:
A proton therapy machine that rotates around you. If you’re undergoing proton therapy with a machine called a gantry, you’ll be placed on a table that is slowly slid into the circular opening of the machine. The machine rotates around you to direct proton beams at precise points on your body.
A proton therapy machine that doesn’t move. If you’re undergoing proton therapy with a fixed-beam machine, the table you’re positioned on will move and the proton therapy machine will remain still. The movement of your table during treatment is controlled remotely by your radiation therapy team. How often your table moves during treatment depends on your situation.
You won’t be able to feel the radiation during your proton therapy treatment.
After proton therapy
Once your treatment session is complete, you can go about your day. You won’t be radioactive or give off radiation.
Side effects of radiation usually develop over time. You may experience few side effects at first. But after several treatments you may experience fatigue, which can make it feel like your usual activities take more energy or that you have little energy for everyday tasks. You may also notice a sunburn-like skin redness in the area where the proton beams are directed.
Results
Your doctor may recommend periodic imaging tests during and after your proton therapy to determine whether your cancer is responding to the treatments. How often you’ll undergo scans depends on your situation.
ASK YOUR DOCTOR WHAT YOUR OPTIONS ARE BEFORE YOU DECIDE ON A TREATMENT.
So much to be discovered in the world of CBD treatments. As soon as we all get away from the stigma that has been placed on a wonderful plant that can help with so many illnesses in so many ways.
Other countries have been testing and experimenting with their patients and CBD for many years, since the early 1920’s. Some say the Egyptians treated illnesses with CBD Hemp Marijuana dates back 3000 years. During the early years of this planet they used herbs and plants native to their areas to use as medicine. This plant was placed on this earth for a reason. Every plant on this earth has a medicinal use of some sort. Some we can even use as poison to kill off bad cells in our bodies. Natural medicine is the answer for so many medical uses .
It was prohibition that caused the medical society to put CBD Hemp Tinctures on the back burner and call it “A MONSTER” that created people to act crazy. We all know that was Alcohol and is to this day and not CBD , Marijuana, Hemp, Grass, Pot and Etc nicknames.
Actually all products and Bi-Products of THC does not make the people go all crazy. Actually opposite of that. They are very mellow and avoid any type of aggressive behavior unlike what we see with alcohol.
Non-Psychoactive
CBD is non-psychoactive because it does not act on the same pathways as the Psychoactive counterparts. These pathways in the brain, called CB1 receptors, are responsible for the psychoactive effects. The .3% or less standard has been established by the FDA as a trace amount with no psychoactive impacts on the human brain.
Cannabidiol (CBD) is a naturally occurring cannabinoid constituent of cannabis. It was discovered in 1940 and initially thought not to be pharmaceutically active. It is one of at least 113 cannabinoids identified in hemp plants, accounting for up to 40% of the plant’s extract. As of 2018 in the United States, Food and Drug Administration approval of cannabidiol as a prescription drug called Epidiolex for medical uses has been limited to two rare forms of childhood epilepsy.
Cannabidiol can be taken into the body in multiple different ways, including by inhalation of cannabis smoke or vapor, as an aerosol spray into the cheek, and by mouth. It may be supplied as an oil containing only CBD as the active ingredient (no added THC or terpenes), a full-plant CBD-dominant hemp extract oil, capsules, dried cannabis, or as a prescription liquid solution.
Crystal Isolates is a high-end vapor liquid and oral drops infused with premium CBD rich hemp oil.
The research continues after several people have died from vaping THC and Vaping.
Side effects of CBD include sleepiness, decreased appetite, diarrhea, fatigue, malaise, weakness, sleeping problems, and others. It does not have intoxicating effects like those caused by THC, and may have an opposing effect on disordered thinking and anxiety produced by THC. CBD has been found to interact with a variety of different biological targets, including cannabinoid receptors and other neurotransmitter receptors. The mechanism of action of CBD in terms of its psychoactive and therapeutic effects is not fully clear.
Are you in need of some sleep? Edibles are a wonderful way to get your medicine dispensed so you can get a good nights rest. Many are available in todays market.
PLEASE RESEARCH YOUR PRODUCTS BEFORE YOU CONSUME ANY TYPE OF THC OR CBD OIL.
CDC reports that Vitamin E Acetate could be responsible for the deaths of 54 as of December 20, 2019…
CDC is confident that Vitamin E acetate is strongly linked to the EVALI outbreak. In a second report in the New England Journal of Medicine, CDC scientists found Vitamin E acetate in lung fluid washings, what we call bronchioloalveolar lavage samples in 48 of 51 samples of patients with EVALI but not in a variety of comparison patient groups. The patients with EVALI came from 16 different states, suggesting this was not a single local supplier of tainted products. These expanded patient clinical specimen results are consistent with previous work including identification by FDA and others of Vitamin E acetate in THC-containing products collected from patients with EVALI, as well as Minnesota’s recent report that Vitamin E acetate was in seized THC products from 2019 but not in any samples from 2018.
Given all of these findings, including today’s study, we can conclude that what I call the explosive outbreak of cases of EVALI can be attributed to exposure to THC-containing vaping products that also contained Vitamin E acetate. I want to stress that this does not mean that there are not other substances in e-cigarette or vaping products that have or are capable of causing lung injury. We know that a persistent small proportion of EVALI cases do not report use of THC-containing vaping products.
Key Facts about Use of E-Cigarette, or Vaping, Products
Electronic cigarettes—or e-cigarettes—are also called vapes, e-hookahs, vape pens, tank systems, mods, and electronic nicotine delivery systems (ENDS).
Using an e-cigarette is commonly called vaping.
E-cigarettes work by heating a liquid to produce an aerosol that users inhale into their lungs.
The liquid can contain: nicotine, tetrahydrocannabinol (THC) and cannabinoid (CBD) oils, and other substances, flavorings, and additives. THC is the psychoactive mind-altering compound of marijuana that produces the “high.”
Some of these products contain antifreeze / engine coolant. These products are harmful and can cause death if used improperly. Prolonged exposure or high concentrations of vapor or mist may cause mild irritation of the respiratory respiratory and headache, dizziness, nausea, vomiting, drowsiness, disturbances of the central nervous system, involuntary eye irritation. If swallowed may cause death if not given emergency services.
“I’m too young to worry about heart disease.” How you live now affects your risk for cardiovascular diseases later in life. As early as childhood and adolescence, plaque can start accumulating in the arteries and later lead to clogged arteries. One in three Americans has cardiovascular disease, but not all of them are senior citizens. Even young and middle-aged people can develop heart problems – especially now that obesity, type 2 diabetes and other risk factors are becoming more common at a younger age.
“I’d know if I had high blood pressure because there would be warning signs.”High blood pressure is called the “silent killer” because you don’t usually know you have it. You may never experience symptoms, so don’t wait for your body to alert you that there’s a problem. The way to know if you have high blood pressure is to check your numbers with a simple blood pressure test. Early treatment of high blood pressure is critical because, if left untreated, it can cause heart attack, stroke, kidney damage and other serious health problems. Learn how high blood pressure is diagnosed.
“I’ll know when I’m having a heart attack because I’ll have chest pain.” Not necessarily. Although it’s common to have chest pain or discomfort, a heart attack may cause subtle symptoms. These include shortness of breath, nausea, feeling lightheaded, and pain or discomfort in one or both arms, the jaw, neck or back. Even if you’re not sure it’s a heart attack, call 911 immediately. Learn you risk of heart attack today!
“Diabetes won’t threaten my heart as long as I take my medication.”Treating diabetes can help reduce your risk for or delay the development of cardiovascular diseases. But even when blood sugar levels are under control, you’re still at increased risk for heart disease and stroke. That’s because the risk factors that contribute to diabetes onset also make you more likely to develop cardiovascular disease. These overlapping risk factors include high blood pressure, overweight and obesity, physical inactivity and smoking.
“Heart disease runs in my family, so there’s nothing I can do to prevent it.” Although people with a family history of heart disease are at higher risk, you can take steps to dramatically reduce your risk. Create an action plan to keep your heart healthy by tackling these to-dos: get active; control cholesterol; eat better; manage blood pressure; maintain a healthy weight; control blood sugar; and stop smoking.
“I don’t need to have my cholesterol checked until I’m middle-aged.” The American Heart Association recommends you start getting your cholesterol checked every 5 years starting at age 20. It’s a good idea to start having a cholesterol test even earlier if your family has a history of heart disease. Children in these families can have high cholesterol levels, putting them at increased risk for developing heart disease as adults. You can help yourself and your family by eating a healthy diet and exercising regularly.
“Heart failure means the heart stops beating.” The heart suddenly stops beating during cardiac arrest, not heart failure. With heart failure, the heart keeps working, but it doesn’t pump blood as well as it should. It can cause shortness of breath, swelling in the feet and ankles or persistent coughing and wheezing. During cardiac arrest, a person loses consciousness and stops normal breathing.
“This pain in my legs must be a sign of aging. I’m sure it has nothing to do with my heart.” Leg pain felt in the muscles could be a sign of a condition called peripheral artery disease. PAD results from blocked arteries in the legs caused by plaque buildup. The risk for heart attack or stroke increases for people with PAD.
“My heart is beating really fast. I must be having a heart attack.” Some variation in your heart rate is normal. Your heart rate speeds up during exercise or when you get excited, and slows down when you’re sleeping. Most of the time, a change in your heartbeat is nothing to worry about. But sometimes, it can be a sign of arrhythmia, an abnormal or irregular heartbeat. Most arrhythmias are harmless, but some can last long enough to impact how well the heart works and require treatment.
“I should avoid exercise after having a heart attack.” No! As soon as possible, get moving with a plan approved for you! Research shows that heart attack survivors who are regularly physically active and make other heart-healthy changes live longer than those who don’t. People with chronic conditions typically find that moderate-intensity activity is safe and beneficial. The American Heart Association recommends at least two and a half hours of moderate intensity physical activity each week For Overall Cardiovascular Health. Find the help you need by joining a cardiac rehabilitation program, but first consult your healthcare provider for advice on developing a physical activity plan tailored to your needs.
Vitamin E acetate is used as an additive, most notably as a thickening agent in THC-containing e-cigarette, or vaping, products.
Vitamin E is a vitamin found in many foods, including vegetable oils, cereals, meat, fruits, and vegetables. It is also available as a dietary supplement and in many cosmetic products, like skin creams.
Vitamin E acetate usually does not cause harm when ingested as a vitamin supplement or applied to the skin. However, previous research suggests that when vitamin E acetate is inhaled, it may interfere with normal lung functioning.
Any of these products pictured here may contain dangerous substances that can kill you!!!
Latest Outbreak Information From The CDC:
This complex investigation spans all states, involves over 2,500 patients, and a wide variety of brands and substances and e-cigarette, or vaping, products.
As of December 3, 2019, CDC is only reporting hospitalized EVALI cases and EVALI deaths regardless of hospitalization status. CDC has removed non-hospitalized cases from previously reported case counts. See Public Health Reporting for more information.
As of December 17, 2019, a total of 2,506 cases of hospitalized e-cigarette, or vaping, product use-associated lung injury (EVALI) have been reported to CDC from 50 states, the District of Columbia, and two U.S. territories (Puerto Rico and U.S. Virgin Islands).
Fifty-four deaths have been confirmed in 27 states and the District of Columbia (as of December 17, 2019): Alabama, California, Connecticut, Delaware, District of Columbia, Florida, Georgia, Illinois, Indiana, Kansas, Louisiana, Massachusetts, Michigan, Minnesota, Mississippi, Missouri, Montana, Nebraska, New Jersey, New York, Oregon, Pennsylvania, Rhode Island, South Carolina, Tennessee, Texas, Utah, and Virginia
The median age of deceased patients was 52 years and ranged from 17 through 75 years (as of December 17, 2019).
More deaths are currently under investigation.
Data suggest the outbreak peaked in September 2019. However, states continue to report new cases, including deaths, to CDC on a weekly basis.
Among cases of hospitalized EVALI patients reported to CDC with available data (as of December 3, 2019): 67% were male (among 2,155 patients with data on sex)
78% were under 35 years old, with a median age of 24 years and age range from 13 to 77 years (among 2,159 patients with data on age)
By age group category: 16% of patients were under 18 years old;
38% of patients were 18 to 24 years old;
24% of patients were 25 to 34 years old; and
23% of patients were 35 years or older.
1,782 hospitalized patients had complete information* on substances used in e-cigarette, or vaping, products in the 3 months prior to symptom onset, of whom (as of December 3, 2019): 80% reported using THC-containing products; 35% reported exclusive use of THC-containing products.
54% reported using nicotine-containing products; 13% reported exclusive use of nicotine-containing products.
12% reported using cannabidiol (CBD)-containing products; 1% reported exclusive use of cannabidiol (CBD)-containing products.
40% reported both THC- and nicotine-containing product use.
5% reported no THC-, nicotine-, or CBD-containing product use.
Among hospitalized EVALI patients who reported using THC-containing e-cigarette, or vaping product brands: The most commonly reported product brand included Dank vapes (56%), followed by TKO (15%), Smart Cart (13%), and Rove (12%). However, regional differences in THC-containing product use were noted.
CDC Laboratory Findings Reported November 8, 2019:
Analyses of bronchoalveolar lavage (BAL) fluid samples (fluid samples collected from the lungs) of patients with e-cigarette, or vaping, product use-associated lung injury (EVALI) identified vitamin E acetate, an additive in some THC-containing e-cigarette, or vaping, products.
CDC laboratory test results of BAL fluid samples from 29 patients submitted to CDC from 10 states found vitamin E acetate in all of the samples.
THC was identified in 82% of the samples and nicotine was identified in 62% of the samples.
CDC tested for a range of other chemicals that might be found in e-cigarette, or vaping, products, including plant oils, petroleum distillates like mineral oil, MCT (medium chain triglyceride) oil, and terpenes (which are compounds found in or added to THC products). None of these chemicals of concern were detected in the BAL fluid samples tested.
This is the first time that we have detected a chemical of concern in biologic samples from patients with these lung injuries. These findings provide direct evidence of vitamin E acetate at the primary site of injury within the lungs.
These findings complement the ongoing work of FDAexternal icon and some state public health laboratories to characterize e-liquid exposures and inform the ongoing multistate outbreak.
Any of these products pictured here can kill you !!!
About the Outbreak:
CDC is only reporting hospitalized EVALI cases and EVALI deaths regardless of hospitalization status. CDC has removed nonhospitalized cases from previously reported case counts. See Public Health Reporting for more information.
As of December 17, 2019, a total of 2,506 hospitalized EVALI cases have been reported to CDC from all 50 states, the District of Columbia, and two U.S. territories (Puerto Rico and U.S. Virgin Islands).
Fifty-four deaths have been confirmed in 27 states and the District of Columbia (as of December 17, 2019).
Although the number of reported cases appears to be declining, states are still reporting new hospitalized EVALI cases to CDC on a weekly basis and should remain vigilant with EVALI case finding and reporting.
About Patient Exposure:
All EVALI patients have reported a history of using e-cigarette, or vaping, products.
Vitamin E acetate has been identified as a chemical of concern among people with e-cigarette, or vaping, product use-associated lung injury (EVALI).
THC is present in most of the samples tested by FDA to date, and most patients report a history of using THC-containing products.
The latest national and state findings suggest THC-containing e-cigarette, or vaping, products, particularly from informal sources like friends, family, or in-person or online dealers, are linked to most of the cases and play a major role in the outbreak.
CDC has analyzed national data on use of THC-containing product brands by EVALI patients.
Overall, 152 different THC-containing product brands were reported by EVALI patients.
Dank Vapes, a class of largely counterfeit THC-containing products of unknown origin, was the most commonly reported product brand used by patients nationwide, although there are regional differences. While Dank Vapes was most commonly reported in the Northeast and South, TKO and Smart Cart brands were more commonly reported by patients in the West and Rove was more common in the Midwest.
The data further support that EVALI is associated with THC-containing products and that it is not likely associated with a single THC-containing product brand.
What We Don’t Know
While it appears that vitamin E acetate is associated with EVALI, there are many different substances and product sources that are being investigated, and there may be more than one cause.
What CDC Recommends
CDC and FDA recommend that people should not use THC-containing e-cigarette, or vaping, products, particularly from informal sources like friends, family, or in-person or online sellers.
Vitamin E acetate should not be added to e-cigarette, or vaping, products. Additionally, people should not add any other substances not intended by the manufacturer to products, including products purchased through retail establishments.
While it appears that vitamin E acetate is associated with EVALI, there are many different substances and product sources that are being investigated, and there may be more than one cause. Therefore, the best way for people to ensure that they are not at risk while the investigation continues is to consider refraining from the use of all e-cigarette, or vaping, products.
Adults using e-cigarettes or vaping products as an alternative to cigarettes should not go back to smoking; they should weigh all available information and consider utilizing FDA-approved cessation medicationsexternal icon. They should contact their healthcare provider if they need help quitting tobacco products, including e-cigarettes.
Adults who continue to use an e-cigarette, or vaping, product should carefully monitor themselves for symptoms and see a healthcare provider immediately if they develop symptoms like those reported in this outbreak.
If you are concerned about your health after using an e-cigarette, or vaping, product, contact your healthcare provider, or local poison control center at 1-800-222-1222.
Adults with ongoing cannabis (marijuana) use that leads to significant impairment or distress should seek out evidence-based behavioral treatment.
Effective treatments are available, and recovery is possible. A number of therapy-based treatments such as cognitive-behavioral therapy, contingency management, motivational enhancement therapy, and multi-dimensional family therapy have been shown to be effective.
For adults currently using marijuana/THC-containing e-cigarette, or vaping, products for medical use: We do not know if there are different health effects of using different forms of marijuana, such as smoking, vaping, and edibles, or whether transitioning from one form to another might reduce harm. Talk with your healthcare provider about other available treatment options for the conditions.
Regardless of the ongoing investigation:
E-cigarette, or vaping, products should never be used by youths, young adults, or women who are pregnant.
Adults who do not currently use tobacco products should not start using e-cigarette, or vaping, products. There is no safe tobacco product. All tobacco products, including e-cigarettes, carry a risk.
THC use has been associated with a wide range of health effects, particularly with prolonged frequent use. The best way to avoid potentially harmful effects is to not use THC-containing e-cigarette, or vaping, products. Persons engaging in ongoing cannabis (marijuana) use that leads to significant impairment or distress should seek evidence-based treatment by a healthcare provider.
Flu is caused by influenza virus of Class A, B and C. Flu spreads directly or indirectly from airborne droplets produced during sneezing or coughing.
Following are the symptoms of flu:
Fever
Malaise
Headache
Runny nose
Postnasal drip
Sneezing
Reduced sense of smell
Metallic taste in mouth
Chills
Cough
Body pain or muscle pain
Sore throat
Take Three Actions to Protect Against Flu
Get Vaccinated
Take preventive steps
Get Treatment
Preventive Steps You Can Take NOW
Try to avoid close contact with sick people.
While sick, limit contact with others as much as possible to keep from infecting them.
If you are sick with flu-like illness, CDC recommends that you stay home for at least 24 hours after your fever is gone except to get medical care or for other necessities. (Your fever should be gone for 24 hours without the use of a fever-reducing medicine.)
Cover your nose and mouth with a tissue when you cough or sneeze. After using a tissue, throw it in the trash and wash your hands.
Wash your hands often with soap and water. If soap and water are not available, use an alcohol-based hand rub.
Avoid touching your eyes, nose and mouth. Germs spread this way.
Clean and disinfect surfaces and objects that may be contaminated with germs like flu.
Treatments
Most of the time flu goes away without treatment. Taking medication can help relieve symptoms. Bed rest will help in faster recovery. Medication
Antiviral: This is used for treat specific viral infections. Oseltamivir · Zanamivir
Monterey Bay Aquarium Research Institute researchers found thousands of holes covering a potential wind-energy farm site off California’s coast, and they aren’t sure what caused them.
During a recent survey of the deep seafloor off Big Sur, MBARI researchers discovered thousands of mysterious holes or pits in the seafloor. Scientists and resource managers want to understand how these pits formed because this area is the site of a proposed wind-energy farm. Researchers Eve Lundsten and Charles Paull describe their discovery this week at the Fall 2019 meeting of the American Geophysical Union in San Francisco.
The researchers found two different sizes of holes. The larger ones, known as pockmarks, average 175 meters (almost 600 feet) across and five meters (16 feet) deep, and are nearly circular and fairly evenly spaced. Some of these pockmarks were initially discovered by MBARI scientists in 1999 during a seafloor survey using ship-mounted sonar. Over the last few years, additional surveys by MBARI and other organizations revealed over 5,200 pockmarks spread out over 1,300 square kilometers (500 square miles), making this area the largest known pockmark field in North America.
More recently, MBARI conducted detailed seafloor surveys using sonar mounted on autonomous underwater vehicles. These surveys revealed thousands of smaller pits, which they termed micro-depressions. The micro-depressions average just 11 meters (36 feet) across and one meter (three feet) deep. They have steeper sides than the pockmarks and are often elongated in one direction.
Seafloor pockmarks have been found elsewhere around the world, and have been associated with releases of methane gas or other fluids from the seafloor. Such methane releases could potentially cause the seafloor to be unstable, which could pose risks for structures such as offshore oil platforms or wind turbines. However MBARI researchers found no evidence of methane in the sediment or seawater in this region. In fact, sonar data showing layers of seafloor sediments suggest that these pockmarks have been inactive for the last 50,000 years.
Don’t forget… VIDEO BELOW
In contrast to the pockmarks, the micro-depressions formed in relatively young sediment. In addition, almost all of the micro-depressions contain objects such as rocks, kelp holdfasts, bones, trash, or fishing gear. Many micro-depressions also have “tails” of sediment that probably originated within the depression. In many areas, these tails are all oriented in the same direction.
Based on these observations, the researchers hypothesize that the micro-depressions are relatively recent features that were were excavated by local seafloor currents. Because the sediment on the seafloor in this area is so soft and “fluffy,” the researchers speculate that even the movements of fish hiding out in the micro-depressions could stir up the sediment, allowing it to be carried away by currents.
Summarizing this work, Lundsten said, “The pockmarks and micro-depressions in this area are both holes in the seafloor that occur in softer sediments, but they are morphologically distinct. The cause and persistence of the pockmarks still remains a mystery, but we find no evidence they were created from gas or fluid in the seafloor in the recent past. The micro-depressions are recently formed erosional features; they are not ‘incipient pockmarks.’ Overall, a lot more work needs to be done to understand how all these features were formed, and this work is in progress.”
Article by Kim Fulton-Bennett
Original research presentation:
Lundsten, E.M., Paull, C., Caress, D.W, Gwiazda, R., Cochrane, G.R., Walton, M.A.L., Nieminski, N., Commingled Seafloor Pockmarks and Micro Depressions Offshore Big Sur, California, AGU Fall 2019 meeting, talk EP11B-02 (Monday, Dec. 9, 8:20 a.m. Moscone West, Room 3009)
Michigan couple thought they were living in their own pre-Halloween spectacle. They noticed there appeared to scratches on Lilly, their daughter. The scratches would appear after putting her in her crib at night.
But this spooky tale had more to offer. After watching the nanny security camera. What they saw had to be reviewed several times for them to even believe what they saw.
Check out what the reporters have to say on ABC 7 WXYZ Detroit, Michigan
MY COMMENT: OMG… nothing more than simple bazar incident to drive you crazy…. Enjoy the story, I did….
If you are anything like me I didn’t know what my Blood Pressure Level should have been. I quickly learned after having a heart attack.
This blood pressure chart will help you as it did me.
This blood pressure chart can help you figure out if your blood pressure is at a healthy level or if you’ll need to take some steps to improve your numbers.
ideal blood pressure chart 70
Your total blood pressure reading is determined by measuring your systolic and diastolic blood pressures. Systolic blood pressure, the top number, measures the force your heart exerts on the walls of your arteries each time it beats. Diastolic blood pressure, the bottom number, measures the force your heart exerts on the walls of your arteries in between beats.
Blood pressure readings fall into four general categories, ranging from normal to stage 2 high blood pressure (hypertension). The level of your blood pressure determines what kind of treatment you may need. To get an accurate blood pressure measurement, your doctor should evaluate your readings based on the average of two or more blood pressure readings at three or more office visits.
Smokeless tobacco is associated with many health problems.
Using smokeless tobacco:
Can lead to nicotine addiction
Causes cancer of the mouth, esophagus (the passage that connects the throat to the stomach), and pancreas (a gland that helps with digestion and maintaining proper blood sugar levels)
Is associated with diseases of the mouth
Can increase risks for early delivery and stillbirth when used during pregnancy
Can cause nicotine poisoning in children
May increase the risk for death from heart disease and stroke
Using smokeless products can cause serious health problems.
Protect your health; don’t start. If you do use them, quit.
Addiction to Smokeless Tobacco
Smokeless tobacco contains nicotine, which is highly addictive.
Because young people who use smokeless tobacco can become addicted to nicotine, they may be more likely to also become cigarette smokers.
Smokeless Tobacco and Cancer
Many smokeless tobacco products contain cancer-causing chemicals.
The most harmful chemicals are tobacco-specific nitrosamines, which form during the growing, curing, fermenting, and aging of tobacco. The amount of these chemicals varies by product.
The higher the levels of these chemicals, the greater the risk for cancer.
Other chemicals found in tobacco can also cause cancer. These include:
A radioactive element (polonium-210) found in tobacco fertilizer
Chemicals formed when tobacco is cured with heat (polynuclear aromatic hydrocarbons—also known as polycyclic aromatic hydrocarbons)

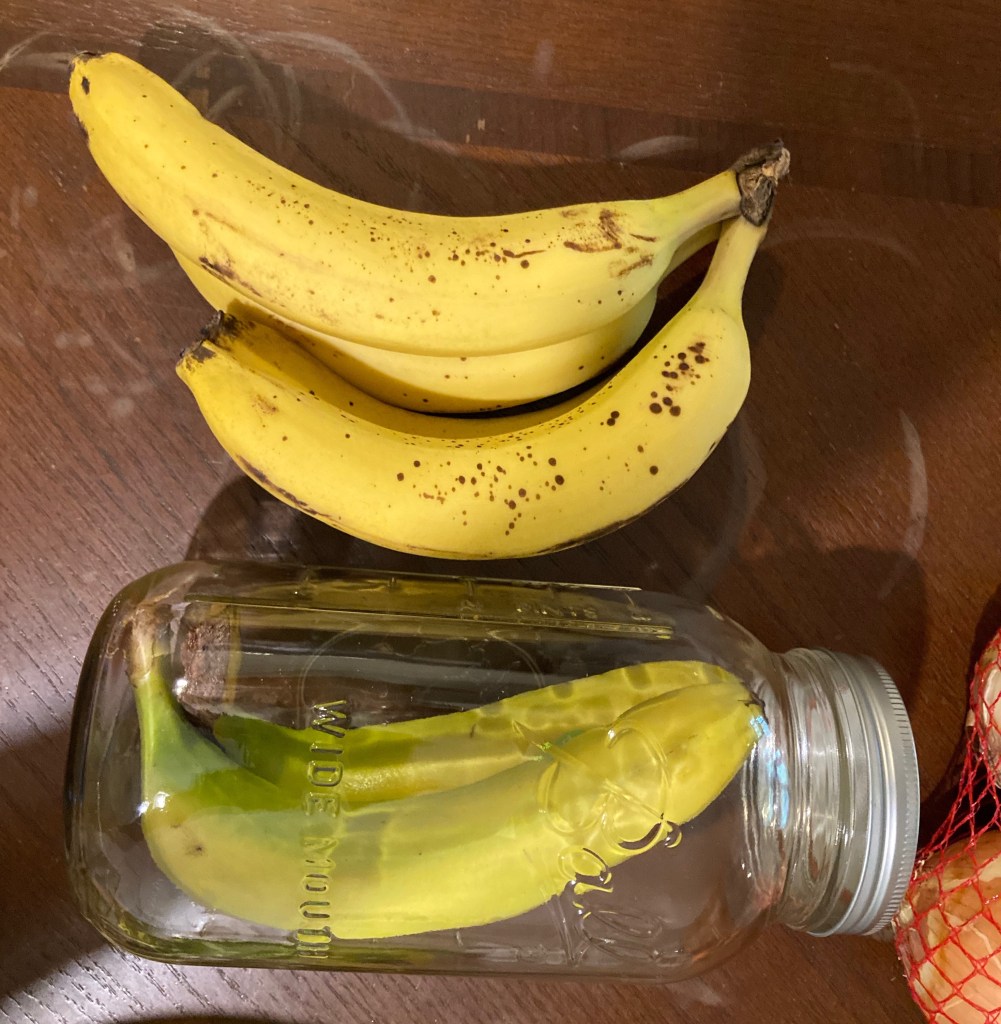







































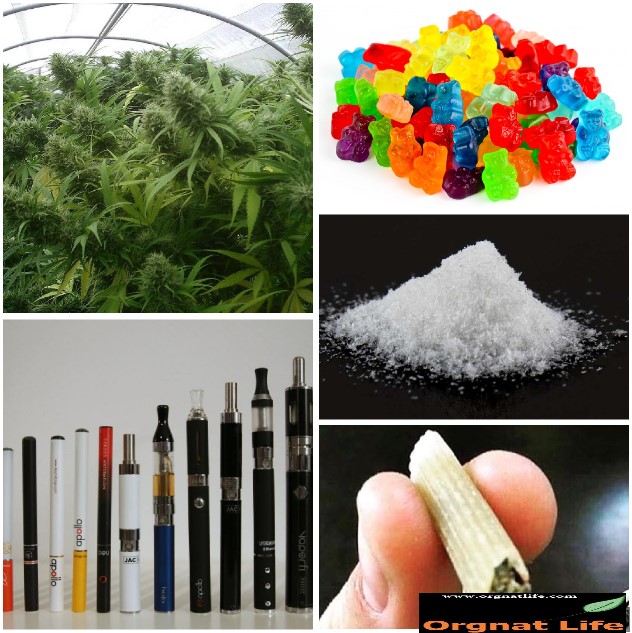









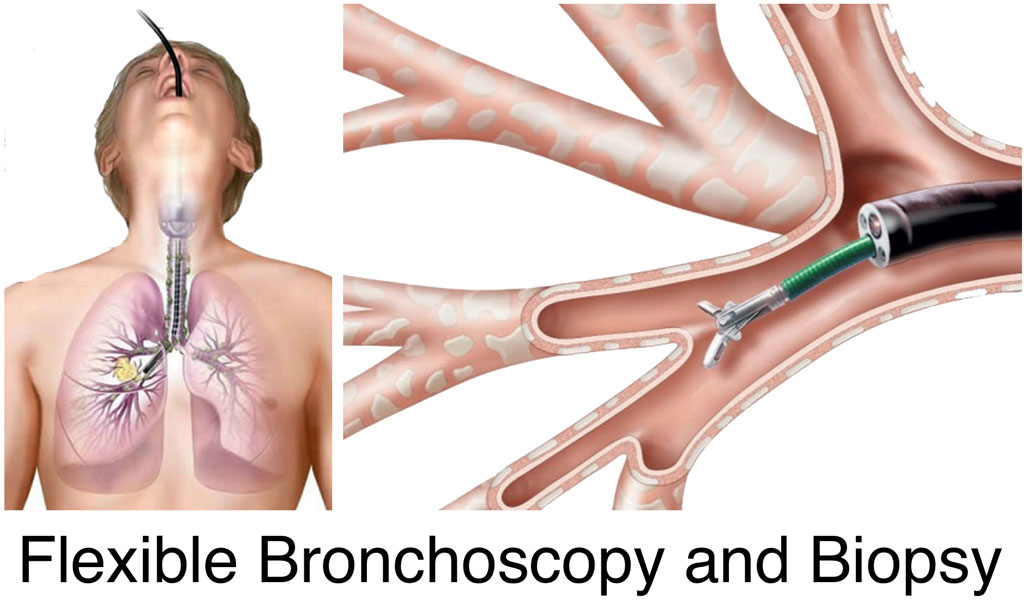
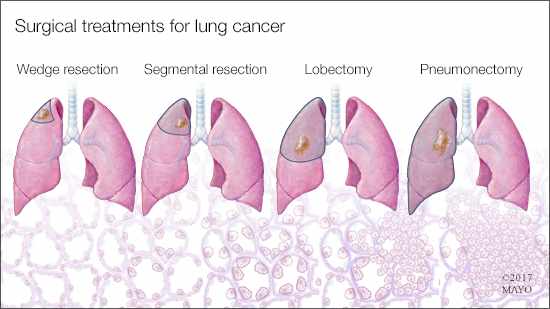











































{kind=link}
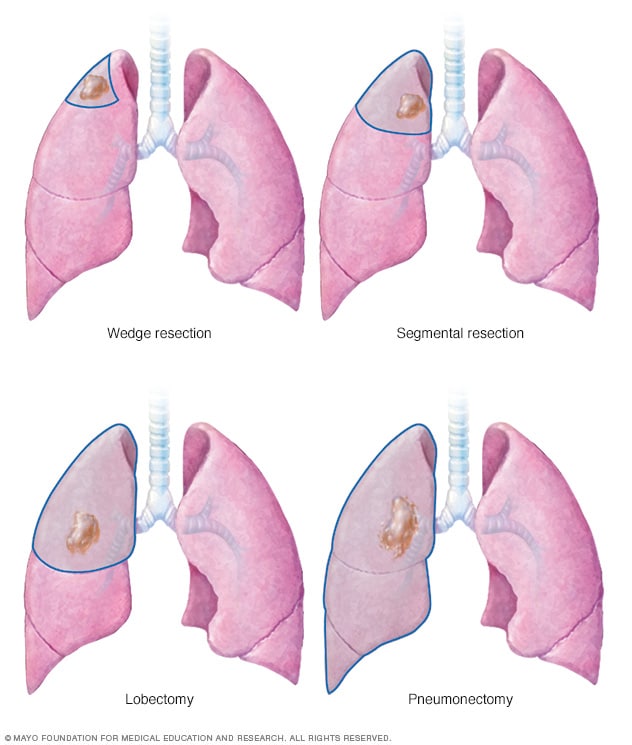{kind=link}