Recently, French Dermatologists revealed that they may have stumbled onto a new COVID-19 symptom.
There are many strains, forms or types of this virus that have all originated from one original virus. It has come in many forms over the years. Animal related to human to slaughtering of millions of chickens throughout the world. Now COVID-19 drops in and kills thousands accross the world. Closes many countries including the USA, right when becoming happy and financially secure once again was actually happening.
We already know the usual symptoms are a dry or constant cough, shortness of breath, fever, flu-like symptoms and headaches. All of these are already proven to be COVID-19 symptoms of a person suffering from the COVID-19 virus.
However, newer symptoms related to the corona virus form COVID-19 are starting to appear as scientists, doctors and experts fighting time to get more information to get a handle on this COVID-19 virus.
Now dermatologists in France have found the virus can cause unusual manifestations on the skin that might signal infection.
According to the New York Post, the French National Union of Dermatologists-Venereologists (SNDV), found dermatological signs like pseudo-frostbite, hives, blisters and persistent redness have been associated with COVID-19. The sudden redness can be painful, said the doctors.
FRANCE – SNDV REPORTS in a press release.: “We are alerting the public and the medical profession in order to detect these potentially contagious patients as quickly as possible. The doctors advised patients to seek medical consultations in the event they experience such symptoms. According to The Hospitalist, skin manifestations were also observed in one-fifth of a group of patients with COVID-19 in the Alessandro Manzoni Hospital in Lecco, in northern Italy.
Honestly, DOES ANYONE KNOW What We Are Dealing With?
REALITY of just how many have died from other virus’s. Why all of a sudden does this virus rate so high on a death scale as “PANDEMIC”?
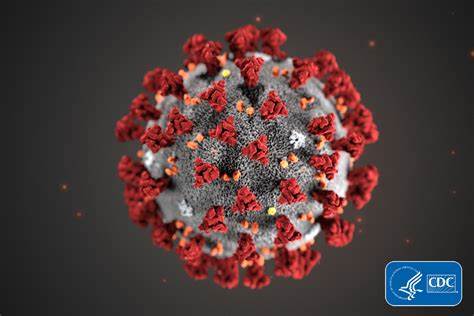
Corona virus has many different strains reported by CDC.
Human Coronavirus Types
Coronaviruses are named for the crown-like spikes on their surface. There are four main sub-groupings of coronaviruses, known as alpha, beta, gamma, and delta.
Human coronaviruses were first identified in the mid-1960s. The seven coronaviruses that can infect people are:
Common human coronaviruses
229E (alpha coronavirus)
NL63 (alpha coronavirus)
OC43 (beta coronavirus)
HKU1 (beta coronavirus)
Other human coronaviruses
MERS-CoV (the beta coronavirus that causes Middle East Respiratory Syndrome, or MERS)
SARS-CoV (the beta coronavirus that causes severe acute respiratory syndrome, or SARS)
People around the world commonly get infected with human coronaviruses 229E, NL63, OC43, and HKU1.
Sometimes coronaviruses that infect animals can evolve and make people sick and become a new human coronavirus. Three recent examples of this are 2019-nCoV, SARS-CoV, and MERS-CoV.
Timeline: Early 1900s –The avian flu is first identified in Italy.
1961 – The H5N1 strain is isolated in birds in South Africa.
December 1983 – Chickens in Pennsylvania and Virginia are exposed to the avian flu and more than five million birds are killed to stop the disease from spreading.
1997 – Eighteenpeople are infected by the H5N1 strain in Hong Kong, six die. These are the first documented cases of human infection. Hong Kong destroys its entire poultry population, 1.5 million birds.
1999 – Two children in Hong Kong are infected by the H9N2 strain.
February 2003 – Eighty-fourpeople in the Netherlands are affected by the H7N7 strain of the virus, one dies.
February 7, 2004 – Twelve thousand chickens are killed in Kent County, Delaware, after they are found to be infected with the H7 virus.
October 7, 2005 – The avian flu reaches Europe. Romanian officials quarantine a village of about 30 people after three dead ducks there test positive for bird flu.
November 12, 2005 – A one-year-old boy in Thailand tests positive for the H5N1 strain of avian influenza.
November 16, 2005 – TheWorld Health Organization confirms two human cases of bird flu in China, including a female poultry worker who died from the H5N1 strain.
November 17, 2005 – Two deaths are confirmed in Indonesia from the H5N1 strain of avian influenza.
January 1, 2006 – A Turkish teenager dies of the H5N1 strain of avian influenza in Istanbul, and later that week, two of his sisters die.
January 17, 2006 – A 15-year-old girl from northern Iraq dies after contracting bird flu.
February 20, 2006 – Vietnam becomes the first country to successfully contain the disease. A country is considered disease-free when no new cases are reported in 21 days.
March 12, 2006 – Officials in Cameroon confirm cases of the H5N1 strain. The avian flu has now reached four African countries.
March 13, 2006 – The avian flu is confirmed by officials in Myanmar.
May 11, 2006 – Djibouti announces its first cases of H5N1 – several birds and one human.
December 20, 2011 – The US Department of Health and Human Services releases a statement saying that the government is urging scientific journals to omit details from research they intend to publish on the transfer of H5N1 among mammals. There is concern that the information could be misused by terrorists.
July 31, 2012 – Scientists announce that H3N8, a new strain of avian flu, caused the death of more than 160 baby seals in New England in 2011.
.January 15, 2016 – The US Department of Agriculture confirms that a commercial turkey farm in Dubois County, Indiana, has tested positive for the H7N8 strain of avian influenza.
January 24, 2017 – Britain’s Department for Environment, Food & Rural Affairs releases a statement confirming that a case of H5N8 avian flu has been detected in a flock of farmed breeding pheasants in Preston, UK. The flock is estimated to contain around 10,000 birds. The statement adds that a number of those birds have died, and the remaining live birds at the premises are being “humanely” killed because of disease.
February 12, 2017 – A number of provinces in China have shut down their live poultry markets to prevent the spread of avian flu after a surge in the number of infections from the H7N9 strain. At least six provinces have reported human cases of H7N9 influenza this year, according to Chinese state media, Xinhua.
On 10 August 2010, the World Health Organization declared the H1N1 influenza pandemic over, saying worldwide flu activity had returned to typical seasonal patterns.
WOW did you ever hear anything hear about that one… Nope Did they shut down the country? NOPE
An influenza pandemic is a global outbreak of a new influenza A virus that is very different from current and recently circulating human seasonal influenza A viruses. Influenza A viruses are constantly changing, making it possible on very rare occasions for non-human influenza viruses to change in such a way that they can infect people easily and spread efficiently from person to person.
Pigs experimentally infected with the strain of swine flu that caused the human pandemic of 2009–10 showed clinical signs of flu within four days, and the virus spread to other uninfected pigs housed with the infected ones and then to humans.
1940s: Thomas Francis, Jr., MD and Jonas Salk, MD serve as lead researchers at the University of Michigan to develop the first inactivated flu vaccine with support from the U.S. Army. Their vaccine uses fertilized chicken eggs in a method that is still used to produce most flu vaccines today. The Army is involved with this research because of their experience with troop loss from flu illness and deaths during WWI. This original vaccine only includes an inactivated influenza A virus.
1940s: First-generation mechanical ventilators become available. These machines support breathing in patients suffering respiratory complications.
1940: Influenza B viruses are discovered.
1942: A bivalent (two component) vaccine that offers protection against influenza A and influenza B viruses is produced after the discovery of influenza B viruses.
1944: Use of cell cultures for virus growth is discovered. This allows viruses to be cultured outside the body for the first time. The ability to culture influenza from respiratory secretions allows diagnosis of influenza.
1945: Inactivated influenza vaccine is licensed for use in civilians.
1942: The Communicable Disease Center (CDC) opens in the old offices of the Malaria Control in War Areas, located on Peachtree Street in Atlanta, Georgia with a satellite campus in Chamblee. Launched with fewer than 400 employees, the organization—today the Centers for Disease Control and Prevention–moves to its current main campus on Clifton Road in Atlanta in 1947 after paying $10 to Emory University for 15 acres of land.
1947: During the seasonal flu epidemic of 1947, investigators determine that changes in the antigenic composition of circulating influenza viruses has rendered existing vaccines ineffective, highlighting the need for continuous surveillance and characterization of circulating flu viruses.
1948: The World Health Organization (WHO) Influenza Centre is established at the National Institute for Medical Research in London. The primary tasks of the organization are to collect and characterize influenza viruses, develop methods for the laboratory diagnosis of influenza virus infections, establish a network of laboratories, and disseminate data accumulated from their investigations.
1950s
1952: The Global Influenza Surveillance and Response System (GISRS) is created by WHO to monitor the evolution of influenza viruses. The GISRS network originally includes 26 laboratories.
1956: The CDC’s Influenza Branch in Atlanta is designated a WHO Collaborating Centre for Surveillance, Epidemiology & Control of Influenza.
1957: A new H2N2 flu virus emerges to trigger a pandemic. There are about 1.1 million deaths globally, with about 116,000 in the U.S.
1960s
1960: In 1960, the US Surgeon General, in response to substantial morbidity and mortality during the 1957–58 pandemic, recommends annual influenza vaccination for people with chronic debilitating disease, people aged 65 years or older, and pregnant women.
1961: An outbreak in South Africa raises possibility of wild birds as a possible reservoir for influenza A viruses.
1962: CDC launches the 122 Cities Mortality Reporting System. Each week, the vital statistics office of 122 cities across the U.S. report the total number of death certificates processed and the number of those for which pneumonia or influenza is listed as an underlying or contributing cause of death by age group. The system is retired in October 2016.
1966: The FDA licenses amantadine, a new antiviral medication, as a prophylactic (preventive medicine) against influenza A. It isn’t effective against influenza B.
1967: Dr. H.G. Pereira and colleagues propose a relationship between human and avian flu viruses after a study shows an antigenic relationship between the 1957 human pandemic A virus and an influenza A virus isolated from a turkey. The study raises the question and triggers the body of work on whether human influenza viruses are of avian origin.
1968: A new H3N2 influenza virus emerges to trigger another pandemic, resulting in roughly 100,000 deaths in the U.S. and 1 million worldwide. Most of those deaths are in people 65 and older. H3N2 viruses circulating today are descendants of the H3N2 virus that emerges in 1968.
1970s
An H1N1 (swine flu) outbreak among recruits at Fort Dix leads to a vaccination program to prevent a pandemic. Within 10 months, roughly 25% of the US population is vaccinated (48 million people), about twice the level needed to provide coverage for the at-risk population. Cases of Guillain-Barre syndrome, a neurologic condition that in rare instances has been associated with vaccination, among vaccine recipients appeared to be in excess of what was expected, so officials determine the vaccination program should be halted. 1981: CDC begins collecting reports of influenza outbreaks from state and territorial epidemiologists.
Initially, infected foreign nationals were turned back at the U.S. border to help prevent additional infections. The number of U.S. deaths from AIDS have declined sharply since the early years of the disease’s presentation domestically. In the United States in 2016, 1.1 million people aged over 13 lived with an HIV infection, of whom 14% were unaware of their infection.
As of 2016, about 675,000 people have died of HIV/AIDS in the U.S. since the beginning of the HIV epidemic, and even today, nearly 13,000 people with AIDS in the United States die each year. [3]
With improved treatments and better prophylaxis against opportunistic infections, death rates have quite significantly declined.[4]
The overall death rate among persons diagnosed with HIV/AIDS in New York City decreased by sixty-two percent from 2001 to 2012.
1990s
1993: The Vaccines for Children (VFC) Program is established as a result of a measles outbreak to provide vaccines at no cost to children whose parents or guardians might not be able to afford them. The program increases the likelihood of children getting recommended vaccinations on schedule.
1993: The costs of influenza vaccine become a covered benefit under Medicare Part B.
1994: Rimantadine, derived from amantadine, is approved by the FDA to treat influenza A.
1996: An avian influenza H5N1 virus is first isolated from a farmed goose in China.
1997: The first human infection with an avian influenza A H5N1 virus is identified in Hong Kong.
1997: FluNet, a web-based flu surveillance tool, is launched by WHO. It is a critical tool for tracking the movement of flu viruses globally. Country data is updated weekly and is publically available.
1998: Influenza virus surveillance in swine, conducted by the US Department of Agriculture, begins in the United States. A virus that is a hybrid of human, bird and swine flu viruses is detected in pigs. This virus becomes the dominant flu virus in U.S. pigs by 1999.
1999: A pandemic planning framework is published by WHO emphasizing the need to enhance influenza surveillance, vaccine production and distribution, antiviral drugs, influenza research and emergency preparedness
1999: The neuraminidase inhibitors oseltamivir (Tamiflu®) and zanamivir (Relenza®) are licensed to treat influenza infection.
2000s
April 2002: The Advisory Committee on Immunization Practices (ACIP) encourages that children 6 to 23 months of age be vaccinated annually against influenza.
2003: Public health officials are concerned about a re-emergence of H5N1 avian influenza reported in China and Vietnam.
June 2003: The first nasal spray flu vaccine is licensed.
2004: The National incident Management System (NIMS) is established to coordinate response for public health incidents that require actions by all levels of government, as well as public, private, and nongovernmental organizations.
2005: The US. Government National Strategy for Pandemic Influenza is published
2005: The entire genome of the 1918 H1N1 pandemic influenza virus is sequenced
2006: CDC stops recommending adamantanes during the 2005-2006 season after high levels of resistance among influenza A viruses. In the US, resistance increased from 1.9% during the 2003-2004 season to 11% in the 2004-2005 season.
2006: The National Strategy for Pandemic Influenza Implementation Plan is published. The document outlines U.S. preparedness and response to prevent the spread of a pandemic.
2007: The American Veterinary Medical Association (AVMA) establishes the One Health initiative Task Force, an effort to attain optimal health for people, animals, and the environment.
2007: The American Medical Association unanimously approves a resolution calling for increased collaboration between human and veterinary medical communities. The term ‘one health,’ which looks at the interactions between animal and human health, enters the medical and scientific lexicon.
2007: The One Health approach is recommended for pandemic preparedness during the International Ministerial Conference on Avian and Pandemic Influenza
2007: FDA approves the first U.S. vaccine for people against an avian influenza A(H5N1) virus.
2007: Human infection with a novel influenza virus is added to the nationally notifiable disease list
2008: ACIP expands its influenza vaccination recommendation to include vaccination of children ages 5-18 years.
2008: HHS Pandemic Influenza Operational Plan is published
2008: CDC receives US Food and Drug Administration approval for a highly sensitive influenza polymerase chain reaction (PCR) assay. These tests can detect influenza with high specificity that enhances diagnosis and treatment options.
2008: The Influenza Reagent Resource (IRR) is established by CDC to provide registered users with reagents, tools, and information to study and detect influenza viruses
April 17, 2009: A new H1N1 virus is detected in the U.S.
CDC begins working to develop a virus (called a candidate vaccine virus) that could be used to make vaccine to protect against this new virus.
April 25, 2009: The World Health Organization (WHO) declares a public health emergency of international concern.
June 11, 2009: WHO officially declares the new 2009 H1N1 outbreak a pandemic.
2009: Physicians use point of care rapid immunoassay tests to provide influenza results within 15 minutes during the H1N1 pandemic
October 5, 2009: The first doses of monovalent H1N1 pandemic vaccine are administered.
2010s
August 10, 2010: WHO declares an end to 2009 H1N1 influenza pandemic.
2010: The ACIP recommends annual influenza vaccination for those 6 months of age and older.
2012: Vaccines containing cell-cultured virus become available. Even though eggs continue to be the primary means of production, cell culture emerges as an alternative method for producing influenza vaccines.
2012: WHO makes first vaccine composition recommendation for a quadrivalent vaccine.
2012: CDC partners with Association of Public Health laboratories to define the optimal right size for influenza virologic surveillance. The project produces right-size calculators; statistical tools that help states determine the optimal amount of influenza testing needed for desired confidence levels of surveillance.
2014: The FDA approves peramivir (Rapivab) to treat influenza in adults. It is the first IV flu medication.
2017: CDC updates guidelines for use of non-pharmaceutical measures to help prevent spread of pandemic influenza based on latest scientific evidence. These are actions that individuals and communities can take to help slow spread of the flu like staying home when sick, covering a cough or sneeze, and frequently washing hands.
A new study suggests that the novel coronavirus(check out the video) COVID-19 can remain in the air for up to three hours, and live on surfaces such as plastic and stainless steel for up to three days.
Pre-existing conditions among people who are more likely to be affected included
diabetes
cancer
chronic lung disease
chronic heart disease
chronic kidney disease
Some infected people had mild symptoms (such as cold-like symptoms) or no symptoms at all.
Coronaviruses are common in many different species of animals, including camels and bats. Rarely, these coronaviruses can evolve and infect humans and then spread between humans. Recent examples of this include SARS-CoV and MERS-CoV.
Most coronaviruses infect animals, but not people. In the future, one or more of these other coronaviruses could potentially evolve and spread to humans, as has happened in the past. We still don’t understand why only certain coronaviruses are able to infect people.
Common human coronaviruses
Common human coronaviruses, including types 229E, NL63, OC43, and HKU1, usually cause mild to moderate upper-respiratory tract illnesses, like the common cold. Most people get infected with these viruses at some point in their lives. These illnesses usually only last for a short amount of time. Symptoms may include
runny nose
headache
cough
sore throat
fever
a general feeling of being unwell
Human coronaviruses can sometimes cause lower-respiratory tract illnesses, such as pneumonia or bronchitis. This is more common in people with cardiopulmonary disease, people with weakened immune systems, infants, and older adults.
Transmission
Human coronaviruses most commonly spread from an infected person to others through
the air by coughing and sneezing
close personal contact, such as touching or shaking hands
touching an object or surface with the virus on it, then touching your mouth, nose, or eyes before washing your hands
rarely, fecal contamination
In the United States, people usually get infected with common human coronaviruses in the fall and winter. However, you can get infected at any time of the year. Most people will get infected with one or more of the common human coronaviruses in their lifetime. Young children are most likely to get infected. However, people can have multiple infections in their lifetime.
Other human coronaviruses
Most people confirmed to have MERS-CoV infection have had severe respiratory illness with symptoms of:
fever
cough
shortness of breath
Some people also had diarrhea and nausea/vomiting. For many people with MERS, more severe complications followed, such as pneumonia and kidney failure. About 3 or 4 out of every 10 people reported with MERS have died. Most of the people who died had a pre-existing medical condition that weakened their immune system, or an underlying medical condition that hadn’t yet been discovered. Medical conditions sometimes weaken people’s immune systems and make them more likely to get sick or have severe illness.
Pre-existing conditions among people who got MERS have included
diabetes
cancer
chronic lung disease
chronic heart disease
chronic kidney disease
Some infected people had mild symptoms (such as cold-like symptoms) or no symptoms at all.
The symptoms of MERS start to appear about 5 or 6 days after a person is exposed, but can range from 2 to 14 days.
The coronavirus that originated in Wuhan, China, raised global concerns but, after a two day meeting, the World Health Organization has issued a statement saying the situation is not yet an emergency of international concern.
Meanwhile, the Centers for Disease Control and Prevention is monitoring the situation and will provide updated information as it becomes available. In addition, Mayo Clinic continues to closely monitor the coronavirus outbreak and says staff is trained and prepared to care for patients, should the need arise. Dr. Pritish Tosh, a Mayo Clinic infectious diseases specialist, says health care providers need to ask patients with respiratory illness and fever about their recent travel. “It’s important we focus on patients with fever and respiratory symptoms, not just for the novel coronavirus, but also for other respiratory viruses that are circulating, such as influenza,” says Dr. Tosh. “Once these patients are identified, they should be given a mask to wear and put into a room where a health care provider can ask them about recent travel.” Dr. Tosh adds, “They may have been to a part of the Middle East where there is ongoing MERS (Middle East respiratory syndrome) infections. They may also have been in Wuhan, China, or been close to someone who has been there.” The coronavirus is in the same family of viruses as SARS (severe acute respiratory syndrome) and MERS.





















{kind=link}